

Introduction: therapy of chronic phase (CP) chronic myeloid leukemia (CML) is based on tyrosine kinase inhibitors (TKIs) in virtually all patients. Three TKIs are approved for first-line therapy in Italy: imatinib and two second-generation (2G) TKIs, dasatinib and nilotinib. Choice of the front-line TKI is based on a combined evaluation of patient's and disease characteristics, age, risk, comorbidities and concomitant medications. Treating physician's preference and, in some cases, economic considerations, particularly after the advent of generic imatinib, may play a role in TKI selection. However, to date, few data are available on TKI use in a whole nation and on the possible drivers of treatment choice. Aim of the present work was to analyse the use of front-line TKI therapy in a large, unselected cohort of Italian CP-CML patients, correlating patient's features to drug choice.
Methods: in the framework of the national Campus CML program, we retrospectively evaluated 1422 patients with CP-CML diagnosed from 2012 and 2019 in 21 haematologic Centres, mostly in academic and/or tertiary hospitals, widespread through the entire Italian territory and treated frontline with imatinib, dasatinib or nilotinib.
Results: median age at diagnosis was 59.9 years [interquartile range (IQR) 47.1 - 71.7], with 317 (22.3%) patients under 45 years, 552 (38.8%) between 45 and 65 years and 553 (38.9%) older than 65 years; 821 (57.7%) patients were males. Among 1364 evaluable patients, CML risk according to Sokal score was low in 540 (39.6%), intermediate in 610 (44.7%) and high in 214 (15.7%) patients respectively; the number at low, intermediate or high risk according to the novel ELTS score among 1325 evaluable patients was 759 (57.3%), 402 (30.3%) and 164 (12.4%) respectively.
Considering comorbidities, 1003 (70.6%) patients had at least one active disease at the time of CML diagnosis, the most common being hypertension (n=547, 38.5%), previous neoplasms (n=185, 13.0%), diabetes (n=150, 10.6%), chronic bronchopulmonary diseases (n=114, 8.0%), acute myocardial infarction (n=95, 6.7%), previous stroke (n=36, 2.5%) and other vascular diseases (n=98, 6.9%). Among 1335 evaluable patients, 813 (60.9%) were taking at least one concomitant medication, with 280 (21.0%) taking 3-5 drugs and 140 (10.5%) taking 6+ drugs at time of TKI start.
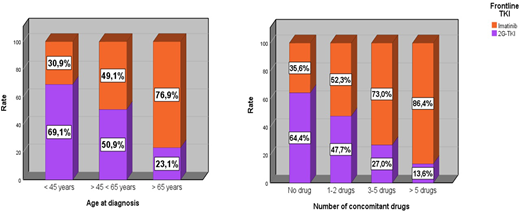
As to the frontline therapy, 794 (55.8%) received imatinib and 628 (44.2%) were treated with 2G-TKIs, (226 dasatinib and 402 nilotinib) respectively. According to age, 2G-TKIs were chosen for majority of patients aged <45 (69.1%) while imatinib was used in 76.9% of patients over 65 (p<0.001). There was a predominance of imatinib use across all Sokal (51.1% in low, 61.3% in intermediate and 51.4% in high) and ELTS (50.3% in low, 60.4% in intermediate and 66.5%) risk categories. We observed a prevalent use of 2G-TKIs in patients presenting with higher WBC counts (55.1% if WBC >100,000/mm3 vs 38.2% if WBC <100,000/mm3; p<0.001), lower Hb (53.8% if Hb <10 g/dl vs 41.9 if Hb >10 g/dl; p=0.001) and bigger spleen (65.1% if spleen >5 cm vs 44.8% if spleen 1-5 cm vs 37.3% if spleen not palpable; p<0.001). There was a decreasing use of 2G-TKIs with higher number of concomitant drugs: 64.4% for 0, 47.7% for 1-2, 27.0% for 3-5 and 13.6% for >5 drugs, respectively (p<0.001). Concordantly, there was a significant higher use of imatinib in patients with hypertension (69.8%), diabetes (70.0%), COPD (73.7%), previous neoplasms (73.0%), AMI (86.3%) or stroke (97.2%) history (p<0.001 for all conditions). Lastly, we observed a wider use of imatinib (61.1%) in patients diagnosed in years 2018-19, compared to those of the period 2012-17 (53.7%; p=0.01). In multivariable analysis, factors correlated with imatinib use were age > 45 years, intermediate or high Sokal risk, presence of some comorbidities (2nd neoplasia and stroke) and number of concomitant medications.
Conclusions: preliminary results of this observational study on almost 1500 patients show that around 55% of newly diagnosed Italian CP-CML patients receive imatinib as front-line therapy, and that the use of 2G-TKI is prevalent in the younger patients and in those with no concomitant clinical conditions. The counterintuitive finding of imatinib prevalence as frontline treatment in high risk patients might be explained by the older age of these patients. Introduction of the generic formulation in 2018 seems to have fostered the use of imatinib.
Breccia:Novartis: Consultancy, Honoraria; Pfizer: Consultancy, Honoraria; Incyte: Consultancy, Honoraria; Abbvie: Consultancy; Bristol-Myers Squibb/Celgene: Consultancy, Honoraria. Cavazzini:Pfize: Honoraria; Incyte: Honoraria; Novartis: Honoraria. Saglio:Bristol-Myers Squibb: Research Funding; Pfizer: Research Funding; Incyte: Research Funding; Novartis: Research Funding; Ariad: Research Funding; Roche: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal